
Bronchiectasis without lower respiratory symptoms in the presence of multisystem anomalies – a clinical clue to diagnose esophageal lung anomaly
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 4 July 2022
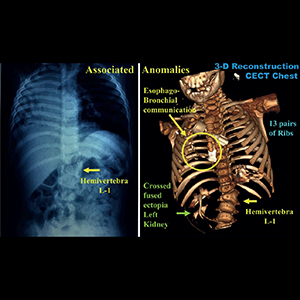
Esophageal lung is a type of Group-II communicating bronchopulmonary foregut malformations (CBPFM) usually diagnosed beyond neonatal period during investigation for recurrent respiratory symptoms and persistent radiographic features suggesting pneumonia or bronchiectasis. In our case, we noticed bronchiectasis and disproportionately severe volume loss in an infant with associated multisystem anomalies in the absence of “significant” lower respiratory tract symptoms. A detailed evaluation with repeat imaging confirmed a Group-II CBPFM, a congenital pathology instead of an infective cause. Pneumonectomy is a more prudent option instead of undertaking major airway reconstruction for the dysplastic “dysfunctional” tissue. Amongst the various associated anomalies reported till now, the associated rib and renal anomalies noted by us have not been described earlier to the best of our knowledge.
Downloads
Leithiser RE, Capitanio MA, Macpherson RI, Wood BP. "Communicating" bronchopulmonary foregut malformations. AJR Am J Roentgenol 1986;146:227. DOI: https://doi.org/10.2214/ajr.146.2.227
Srikanth MS, Ford EG, Stanley P, Mahour GH. Communicating bronchopulmonary foregut malformations: classification and embryogenesis. J Pediatr Surg 1992;27:732-6 DOI: https://doi.org/10.1016/S0022-3468(05)80103-4
Keeley JL, Schairer AE, Brosnan JJ. The anomalous origin of the right main bronchus from the esophagus. Ann Surg 1960;81:641–5. DOI: https://doi.org/10.1097/00000658-196011000-00014
Parelkar SV, Sanghavi BV, Patil SH, et al. Esophageal lung – A rare bronchopulmonary foregut malformation. J Pediatr Surg Case Rep 2014;2:511-4. DOI: https://doi.org/10.1016/j.epsc.2014.10.011
Heithoff KB, Sane SM, Williams HJ. Bronchopulmonary foregut malformations: a unifying etiological concept. AJR Am J Roentgenol 1976;126:46-55. DOI: https://doi.org/10.2214/ajr.126.1.46
Saydam TC, Mychaliska GB, Harrison MR. Esophageal lung with multiple congenital anomalies: conundrums in diagnosis and management. J Pediatr Surg 1999;34:615-8. DOI: https://doi.org/10.1016/S0022-3468(99)90087-8
Sur A, Sardar SK, Paria A. Left sided oesophageal lung: a diagnostic challenge. Case Rep Pediatr 2013;2013:947401. DOI: https://doi.org/10.1155/2013/947401
Yang G, Chen L, Xu C, et al. Congenital bronchopulmonary foregut malformation: systematic review of the literature. BMC Pediatr 2019;19:305. DOI: https://doi.org/10.1186/s12887-019-1686-1
Alsaadi A, Alsufiani HA, Allugmani MD, Gora AF. Esophageal lung with rare associated vascular and anorectal malformations. Radiol Case Rep. 2018;13:444-8. DOI: https://doi.org/10.1016/j.radcr.2018.01.029
Bokka S, Jaiswal AA, Behera BK, et al. Esophageal lung: A rare type of communicating bronchopulmonary foregut malformation, case report with review of literature. J Indian Assoc Pediatr Surg 2015;20:92-4. DOI: https://doi.org/10.4103/0971-9261.151558
Harrell KN, Brent Moss J, Dave Bhattacharya S, Koontz CS. Management of esophageal lung in a patient with VACTERL anomalies. Am Surg 2020;86:1538-40. DOI: https://doi.org/10.1177/0003134820933615
Deshpande A, Patil S, Gupta A, Kothari P. Esophageal lung associated with VACTERL anomaly: a case report. Int J Res Med Sci 2017;5:3243-6. DOI: https://doi.org/10.18203/2320-6012.ijrms20173023
Hu X, Wu L. Esophageal lung in association with pulmonary vascular anomalies. Lung 2018;196:631-2. DOI: https://doi.org/10.1007/s00408-018-0147-1
Katz R, Pitt R, Kim D, Wingrove B. Thoracoscopic pneumonectomy for communicating bronchopulmonary foregut malformation in a 4-month-old child. J Pediatr Surg 2010;45:427-9. DOI: https://doi.org/10.1016/j.jpedsurg.2009.11.045
Matsumoto Y, Ohi R, Hayashi Y, Chiba T. Right pneumonectomy syndrome: report of two cases. Surg Today 1995;25:278-80. DOI: https://doi.org/10.1007/BF00311543
Takamizawa S, Yoshizawa K, Machida M, et al. Successful tracheobronchial reconstruction of communicating bronchopulmonary foregut malformation and long segment congenital tracheal stenosis: a case report. J Pediatr Surg 2012;47:E41-6. DOI: https://doi.org/10.1016/j.jpedsurg.2012.06.009
Berger M, de Cárdenas JAM, Hosseinpour R, de Agustín Asensio JC. Simultaneous correction of esophageal lung and congenital tracheal stenosis: Lessons learned. J Pediatr Surg Case Rep 2013;1:288-92. DOI: https://doi.org/10.1016/j.epsc.2013.07.017
How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.