
Right-sided infective endocarditis and pulmonary embolism: a multicenter study
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 12 April 2022
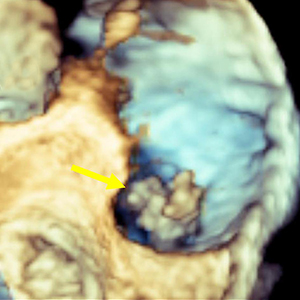
The incidence of right-sided infective endocarditis (RSIE) is steadily increasing and it has been reported to be associated with high risk of embolic events (EE). Aim of our study was to identify the clinical characteristics of patients with RSIE complicated by PE. Indeed, the identification of patients at high risk of significant PE who will benefit from a more aggressive therapeutic strategy may improve the prognosis. From January 2015 to September 2020, 176 patients (Pts) in 6 centers were found to have definite RSIE complicated by PE. Advanced imaging for PE including computed tomography pulmonary angiography (CTPA) was performed in 28 pts (16%) who represent our study group (24 male, mean age 50.6 ±18.29 years). They all underwent transesophageal echocardiography (TEE), in 12 cases (43%) also three-dimensional (3D) TEE, and 27 patients (99%) had both TEE and transthoracic echocardiography (TTE). A total of 53 vegetations (V) were detected. In 18 pts (64%) two or more vegetations were found. Native tricuspid valve was the most frequently involved valve (38 V, 71.7%), followed by catheter (5 V, 9.4%), tricuspid valve prosthesis (4 V, 7.5%), chordae and papillary muscle (2 V, 3.8%) and one vegetation (9%) in each of the following: pulmonic valve, inferior vena cava, eustachian valve, and right atrium. The most common location for vegetations was the anterior leaflet of the tricuspid valve (19 V, 35.8 %) followed by the posterior leaflet (11 V, 20.8%). The most common vegetations morphology was raceme-like shaped (35.8%). Staphylococcus aureus (S. aureus) was the most common causative pathogen (14 pts, 50%). The incidence of PE was very high in patients with vegetation length above 1.5 cm (median 17.6±6.5 mm by TEE). Our results suggest that a routine CTPA should be advised in the presence of vegetations larger than 1.5 cm and with S. aureus infection. This behavior would identify patients at high risk of PE who will benefit from a more aggressive therapeutic strategy, leading to an improvement in the prognosis. Further prospective studies are required to better confirm our hypothesis.
Downloads
Habib G, Hoen B, Tornos, et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur heart J 2009 30:2369–413.
Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021;143:e35-e71. DOI: https://doi.org/10.1161/CIR.0000000000000932
Habib G, Lancellotti P, Antunes MJ, et al. ESC Scientific Document Group. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015;36:3075-128. DOI: https://doi.org/10.1093/eurheartj/ehv319
Habib G, Erba PA, Iung B, et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: a prospective cohort study. Eur Heart J 2019;40:3222‐32.
Di Salvo G, Habib G, Pergola V, et al. Echocardiography predicts embolic events in infective endocarditis. J Am Coll Cardiol 2001;37:1069–76. DOI: https://doi.org/10.1016/S0735-1097(00)01206-7
6 - Utsunomiya H, Berdejo J, Kobayashi S, et al. Evaluation of vegetation size and its relationship with septic pulmonary embolism in tricuspid valve infective endocarditis: a real time 3D TEE study. Echocardiography 2017;34:549-56. DOI: https://doi.org/10.1111/echo.13482
Shmueli H, Thomas F, Flint N, et al. Right-sided infective endocarditis 2020: Challenges and updates in diagnosis and treatment. J Am Heart Assoc 2020;9:e017293. DOI: https://doi.org/10.1161/JAHA.120.017293
Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J 2020;41:543-603. DOI: https://doi.org/10.1093/eurheartj/ehz405
Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2015;28:1-39.e14. DOI: https://doi.org/10.1016/j.echo.2014.10.003
Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr 2010;23:685-713; quiz 786-8.
Zoghbi WA, Adams D, Bonow RO, et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr 2017;30:303-71. DOI: https://doi.org/10.1016/j.echo.2017.01.007
Thuny F, Di Salvo G, Belliard O, et al. Risk of embolism and death in infective endocarditis: prognostic value of echocardiography: a prospective multicenter study. Circulation 2005;112:69–75. DOI: https://doi.org/10.1161/CIRCULATIONAHA.104.493155
Pérez-García CN, Olmos C, Islas F, et al. Morphological characterization of vegetation by real-time three-dimensional transesophageal echocardiography in infective endocarditis: Prognostic impact. Echocardiography 2019;36:742-51. DOI: https://doi.org/10.1111/echo.14293
Lancellotti P, Galiuto L, Albert A, et al. Relative value of clinical and transesophageal echocardiographic variables for risk stratification in patients with infective endocarditis. Clin Cardiol 1998;21:572-8. DOI: https://doi.org/10.1002/clc.4960210808
Berdejo J, Shibayama K, Harada K et al. Evaluation of vegetation size and its relationship with embolism in infective endocarditis: a real-time 3-dimensional transesophageal echocardiography study. Circ Cardiovasc Imaging 2014;7:149–54. DOI: https://doi.org/10.1161/CIRCIMAGING.113.000938
Galzerano D, Kinsara AJ, Di Michele S, et al. Three dimensional transesophageal echocardiography: a missing link in infective endocarditis imaging? Int J Cardiovasc Imaging 2020;36:403-13. DOI: https://doi.org/10.1007/s10554-019-01747-x
Lang RM, Badano LP, Tsang W et al. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. Eur Heart J Cardiovasc Imaging 2012;13:1-46. DOI: https://doi.org/10.1093/ehjci/jer316
Lang RM, Addetia K, Narang A, Mor-Avi V. 3-Dimensional echocardiography: Latest developments and future directions. JACC Cardiovasc Imaging 2018;11:1854-78. DOI: https://doi.org/10.1016/j.jcmg.2018.06.024
How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.